Mako™ Total Knee Replacement Surgery Introduction
The Mako™ Robotic Total Knee System is a highly advanced, consistently, reproducible, precision joint replacement installation system for patients with knee arthritis too advanced for Mako™ Partial Knee replacement. Dr. Buechel is an expert user of the Mako™ Robotic Knee system and has an international surgical experience of over 1,500 Mako™ Robotic knee procedures operating on people from around the world. Dr. Buechel understands which patients are best suited for Partial Knee replacement and which patients’ knee arthritis is too advanced and will benefit from Mako™ Total Knee replacement.
Dr. Buechel’s vast robotic experience allows him to optimize each person’s knee implant installation, utilizing all the tools provided by Mako™ Total Knee to improve the implant’s position, balance, function & longevity, while creating the most “natural feel” for the patient.
Mako™ Total Knee Replacement Features
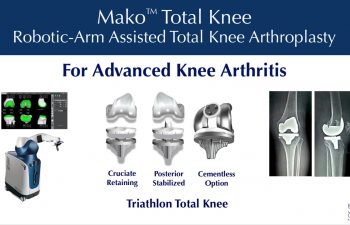
The Mako™ Robotic Total Knee System uses the Stryker Triathlon Knee System implants along with advanced software to optimize each patient’s implant installation. The implant options allow Dr. Buechel to maintain the posterior cruciate ligament (PCL) or substitute for it, when it is not healthy. For some patients, fixation of the implants to the bone will be with cement, for others advanced coatings for biologic fixation can be used without cement.
The Mako™ Total Knee System provides the most accurate way to plan implant placement for each patient customizing the size, position, alignment, and ligament balance to optimize the patient’s function. The Robotic bone preparation provides precision bone cuts and provides safety boundaries protecting the soft tissues, nerves and vessels from injury.

The Benefits of Dr. Buechel’s Mako™ Robotic Total Knee Replacement Surgery
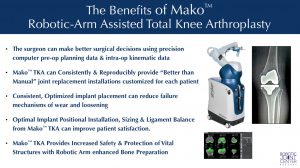 The Mako™ Total Knee System empowers Dr. Buechel with more information, more accurate information, and live dynamic information about size, alignment and balance to make better surgical decisions than with conventional tool systems alone. Optimizing ligament balance, implant position and leg alignment using precision software while making precise, safe bone cuts with the robotic arm assistance benefits each patient by providing them with a customized installation. This translates to a more precisely placed knee replacement optimized for each individual’s personal characteristics producing a more comfortably functioning knee.
The Mako™ Total Knee System empowers Dr. Buechel with more information, more accurate information, and live dynamic information about size, alignment and balance to make better surgical decisions than with conventional tool systems alone. Optimizing ligament balance, implant position and leg alignment using precision software while making precise, safe bone cuts with the robotic arm assistance benefits each patient by providing them with a customized installation. This translates to a more precisely placed knee replacement optimized for each individual’s personal characteristics producing a more comfortably functioning knee.

The Process for a Mako™ Total Knee Replacement
Office Evaluation
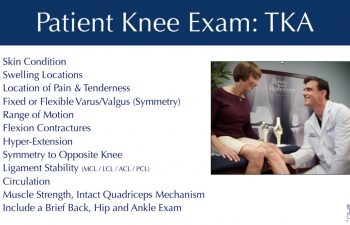
The Office Evaluation prior to surgery is used to review each patient’s symptoms, their knee history, their medical history, perform a physical exam, and to review imaging of the patient’s knee. This evaluation helps Dr. Buechel understand each patient’s situation, confirm that the physical findings align with the history and imaging, which allows Dr. Buechel to confirm the recommended procedure for each patient’s knee problem.
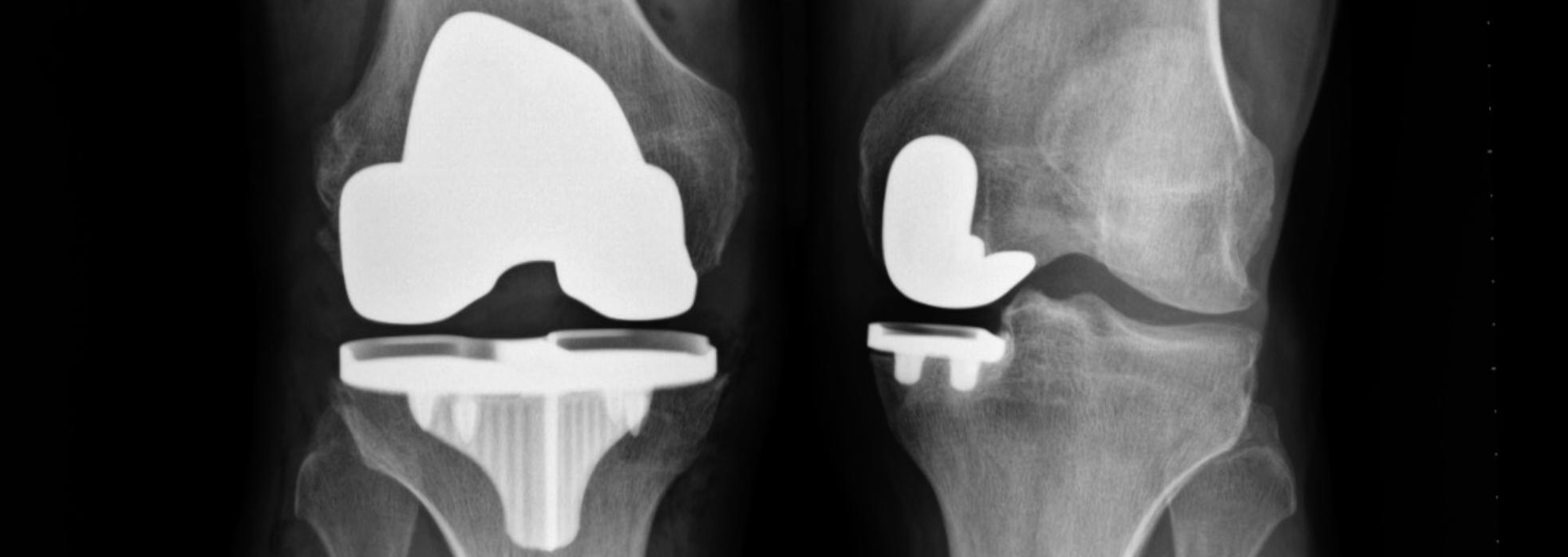
X-Rays for Evaluation of the Knee
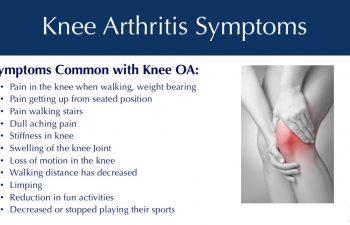
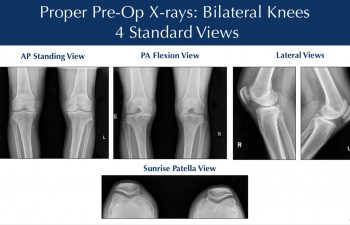
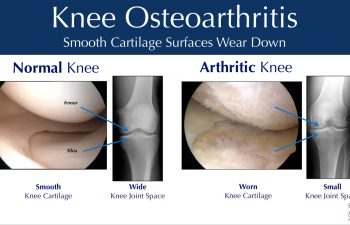
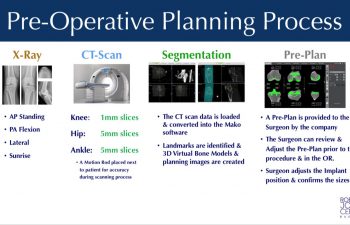
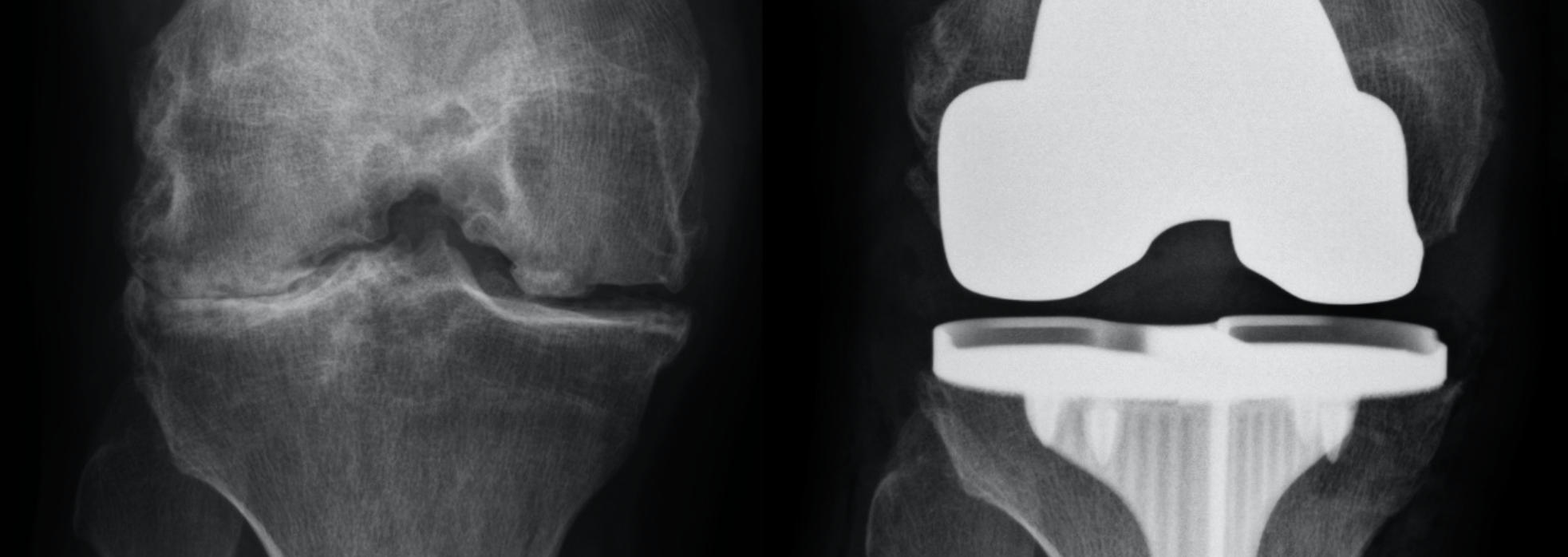
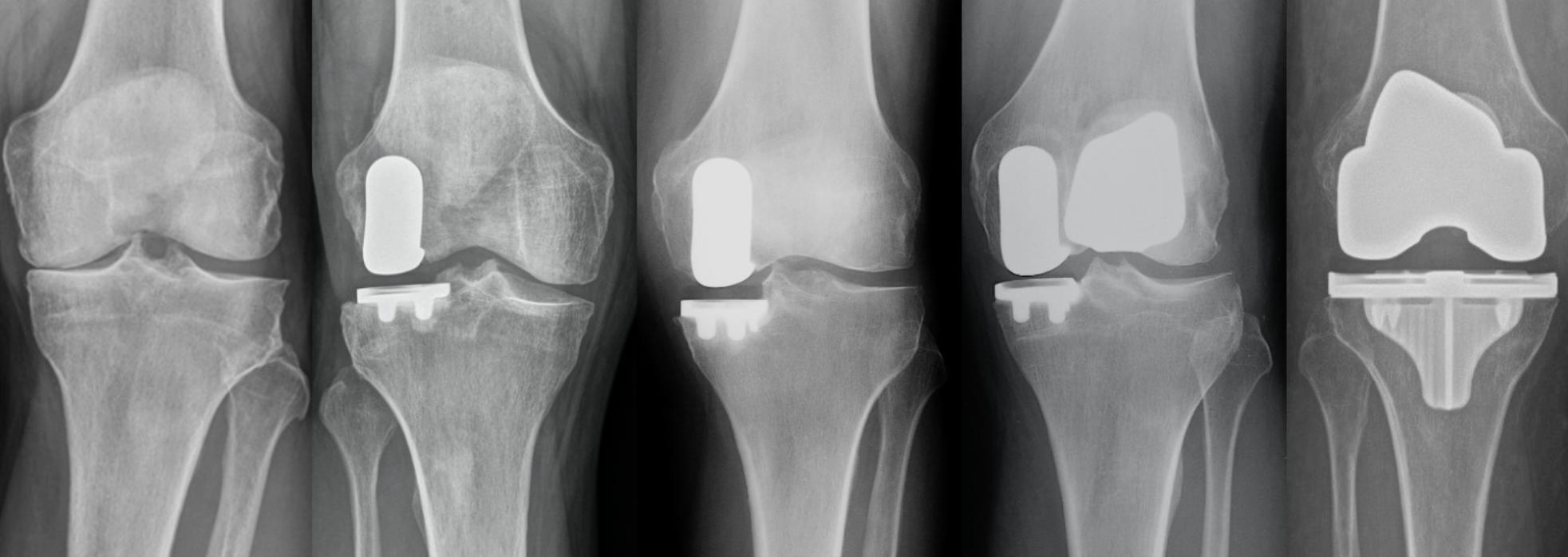
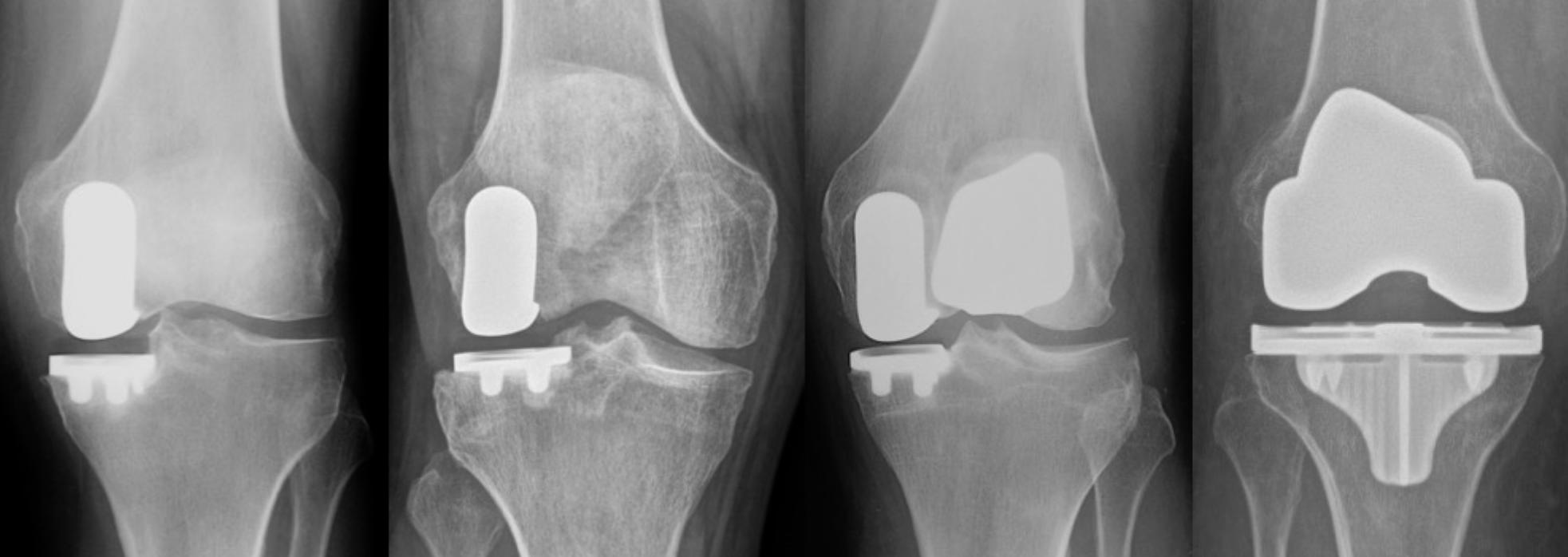
Patients obtain X-rays with 4 views of their knee to look for mild, moderate or severe joint space loss or destruction in one or more compartments from osteoarthritis, rheumatoid arthritis, osteonecrosis or post-traumatic arthritis. These views include a standing Anterior to Posterior View, Standing Posterior to Anterior Flexion View, a Lateral View and a Sunrise View.
If the x-rays and the exam are consistent with partial knee arthritis, then a patient may be a candidate for the Mako™ Partial Knee Resurfacing procedure. If the disease is more advanced, then the Mako™ Total Knee Replacement is offered.

Clinical Indications for Mako™ Total Knee
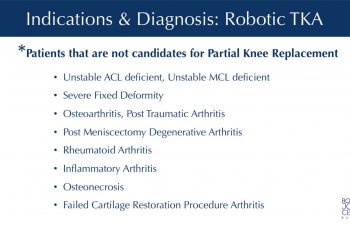
The clinical indication to proceed with Mako™ Robotic Total Knee is determined by a proper diagnosis, an appropriate medical and knee history, Dr. Buechel’s examination that confirms the findings and evaluates the patient’s condition, and imaging studies that support these conclusions. The most common reason for knee replacement surgery is osteoarthritis. Other reasons include: arthritis after meniscectomy, post-traumatic arthritis, osteonecrosis, inflammatory arthritis, osteo-chondral defects, and failed cartilage restoration procedures.
There are a few reasons that Dr. Buechel and other surgeons would recommend against a knee replacement which can include infection history in the knee, some severe deformities or congenital problems, neurologic conditions that make the muscles unable to support the knee, skin problems that can compromise wound healing, some extreme weight conditions, and medical conditions that create too high of a risk for complications.

Pre-Operative Planning for Mako™ Total Knee
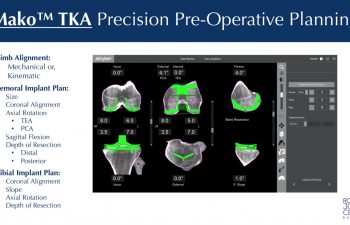
Pre-Planning is the process of preparing for the robotic knee procedure by obtaining precision 3D CT knee imaging data that is loaded into an advanced knee implant software platform. This allows the surgeon to position the virtual knee implants onto the patient specific knee bone models. Pre-planning allows the surgeon to plan the exact size, the implant depth, sagittal, coronal & transverse rotation, posterior slope, and coronal plane alignment of the chosen implants prior to the procedure.
As a critical part of the procedure, preoperative computer planning and evaluation makes a big difference in the efficiency and quality of the surgical procedure to follow, and the outcome. The preoperative CT scan provides enormous benefit to patients & Dr. Buechel. Once the CT data is loaded into the software, Dr. Buechel optimizes the patient’s implant positions based on each patient’s anatomy, with one millimeter and 1degree precision. The anatomic preoperative plan is optimized during surgery from motion data, limb alignment data, and ligament gap analysis to optimize each patient’s individual placement.

Value & Safety Provided by the Mako™ Pre-Op CT
The preoperative CT scans often reveal important information pre-operatively. Large bone spurs, often not seen with imageless systems, are important to know about preoperatively, as they influence implant positioning and balance decisions during surgery, effecting proper joint tension. On the more advanced arthritis cases with lots of large bone spurs, the scans help tremendously in planning & ensuring their removal.
There can be a concern with CT scans related to radiation dosage and its potential detrimental effects. I have been concerned as well, so our radiologists have shared with us that the special protocol for this knee scan delivers a mean effective dose of only ~0.4mSv, which is equivalent to 1.5 months of natural environmental radiation, or 3 x-rays. Therefore, I strongly feel the benefit outweighs the minimal risk.
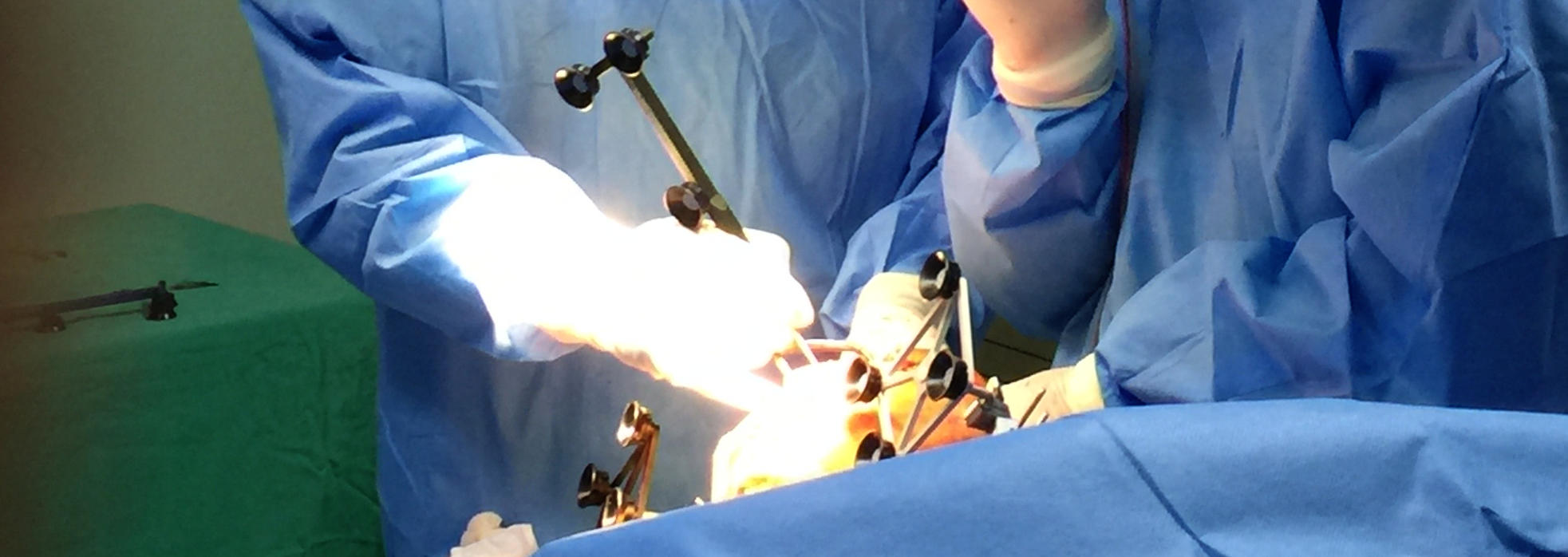
Patient & Robotic Operating Room Setup
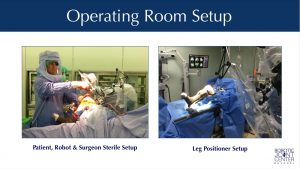 Once the operating room is ready, the patient is brought into the operating room and properly positioned on a comfortable and well-padded operating table. Once the anesthesiologist has completed their preparation of the patient with either a regional or general anesthesia, the patient is sterilely prepared, padded and draped.
Once the operating room is ready, the patient is brought into the operating room and properly positioned on a comfortable and well-padded operating table. Once the anesthesiologist has completed their preparation of the patient with either a regional or general anesthesia, the patient is sterilely prepared, padded and draped.
Incisions & Exposure
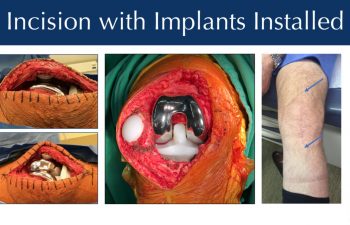
Dr. Buechel’s skin incisions are generally 5-6 inches in length (small to average size). It has been shown in the literature that in total knee surgery mini incisions have compromised the end results of many knee replacements. Therefore, appropriate exposure is my goal so that the skin remains healthy during and after the surgery to ensure proper wound healing, and that the proper bone preparation, bone spur and cement removal is complete, and proper balancing is performed.
Advanced medicines are used to reduce blood loss during, and after surgery. No tourniquets are used to reduce blood clot risk and post-operative pain, electro-cautery knives are used to minimize bleeding during the exposure. Skin adhesives and antibiotic coated barbed suture are used during closure on most patients to hold the tissue edges together better, reduce the risk of external contamination, while allowing patients to shower the next day. You will see the cosmetically acceptable results of this technique in the photo above on a patient just 6 months after surgery.

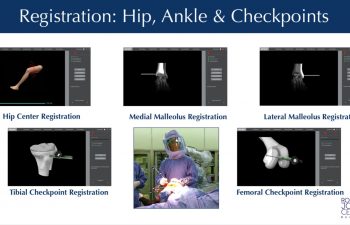
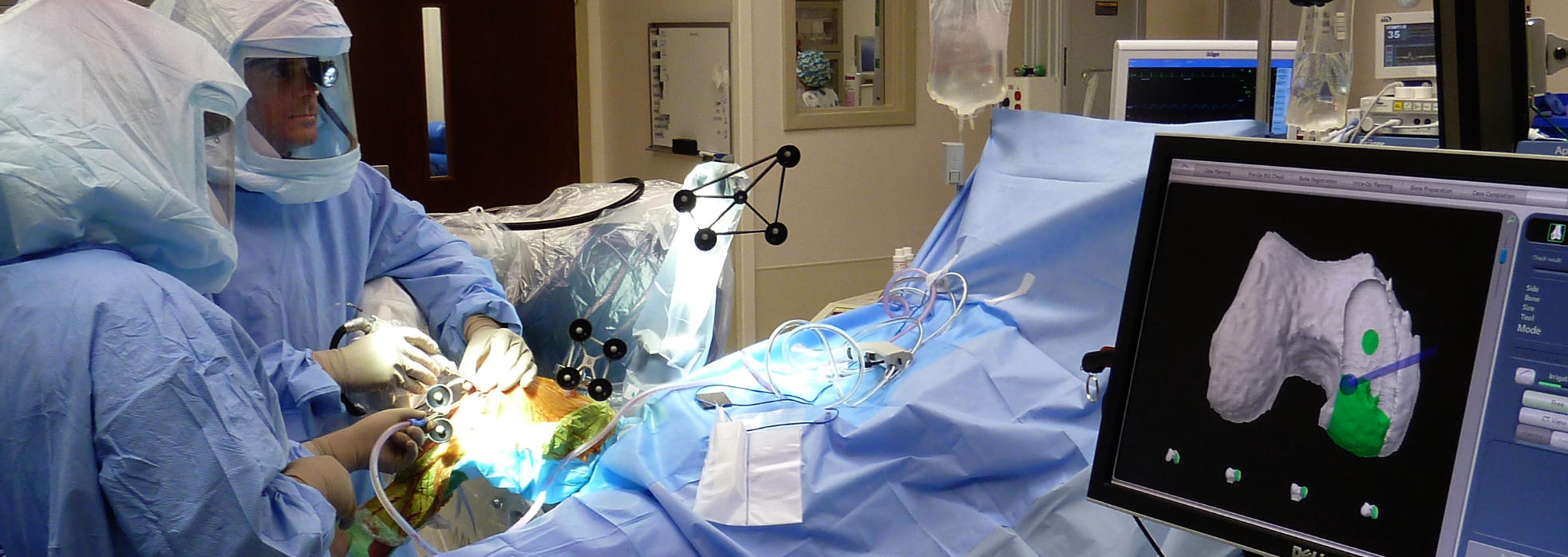
Tracking Arrays & Registration
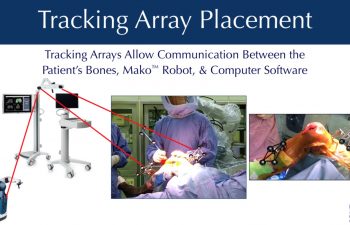
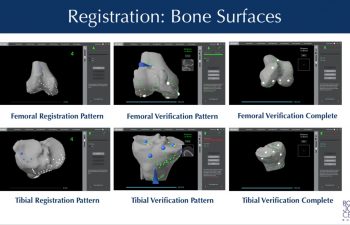
During the procedure, Dr. Buechel places temporary infrared tracking devices called “Arrays”, on the femur and tibia. These allow the computer to “see” the bones moving in the operating room, know the exact position of the robot with its cutting tool, and match the precise location of the bone of the patient to the 3D CT scan plan in the computer. This process is called “Registration”.
Bone Spur Removal in Preparation for Data Collection
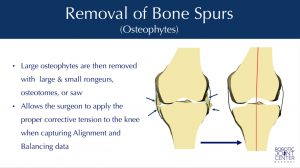 Once the communication has been established by matching the patient to the CT data through the “Registration” process, any overgrown bone spurs can be removed. This is part of the preparation to properly re-tension the knee ligaments, individually re-align the knee, and then collect data to allow for optimal implant planning & positioning.
Once the communication has been established by matching the patient to the CT data through the “Registration” process, any overgrown bone spurs can be removed. This is part of the preparation to properly re-tension the knee ligaments, individually re-align the knee, and then collect data to allow for optimal implant planning & positioning.

Intra-Operative Planning:Data Collection, Functional Planning & Implant Adjustment
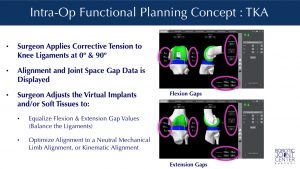 Once the software/patient/robot communication is setup in the operating room, Dr. Buechel bends the knee through a range of motion while he re-tensions the ligaments of the knee and optimizes the angular alignment for each patient. This allows the computer software to present Dr. Buechel with implant dynamic ligament gap analysis and limb alignment data, so he can make virtual adjustments of the implants to optimize their position prior to robotic bone preparation.
Once the software/patient/robot communication is setup in the operating room, Dr. Buechel bends the knee through a range of motion while he re-tensions the ligaments of the knee and optimizes the angular alignment for each patient. This allows the computer software to present Dr. Buechel with implant dynamic ligament gap analysis and limb alignment data, so he can make virtual adjustments of the implants to optimize their position prior to robotic bone preparation.
Understanding how to optimize this data collection process and adjust for different deformities is where Dr. Buechel’s vast experience using the system makes a significant difference.

Mako™ Robotic Bone Preparation
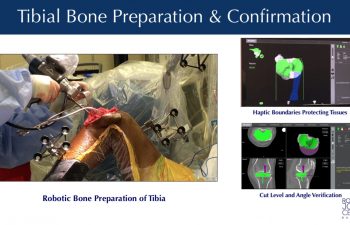
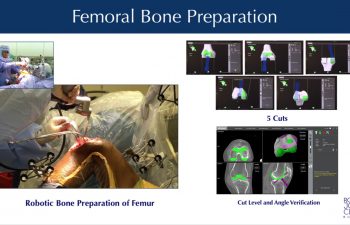
With the intraoperative plan optimized, Dr. Buechel guides the robotic cutting tool (a precision saw) connected to the end of a robotic-arm across the bone surfaces, removing the planned volume of bone resection. The robotic system provides visual, audible and tactile feedback limiting the area of resection to only the planned surface within a millimeter and one degree of the plan. The robotic system creates virtual boundaries like an “invisible wall”, safely and precisely limiting the movement of the cutting tool. Once the bone surface is prepared by the robotic cutting tool, Dr. Buechel then trims and prepares the remaining soft tissues in the joint space in preparation to install the trial implants, and then the final implants.

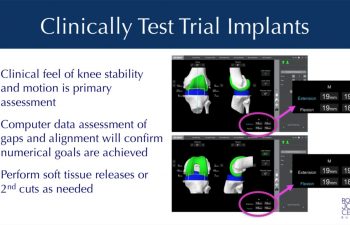
Stryker Triathlon Implant Installation and Verification
The Stryker Trial implants are installed without cement to test the tracking, tension and stability of the knee joint. The computer software allows a review of the alignment, ligament gaps and balance. Adjustments can be made to the soft tissues or through secondary robotic guided bone cuts to optimize any of the parameters to provide the most stable well aligned knee possible.
Once optimal conditions are confirmed with the trials in place, the final implants are opened prepared to be attached to the knee.
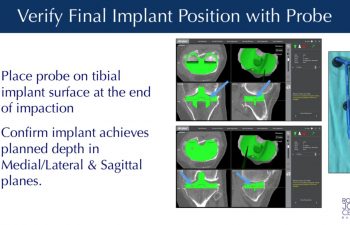
The final implants are installed with or without the use of bone cement, attaching them to the femoral, tibial and patella bones. Probes can be used to verify the precise seating of the implants at their planned locations on the bone.
Wound Closure & Healing Optimization
Dr. Buechel is focused on optimizing wound healing for all of his surgical patients. Therefore, he has recommendations on the entire process from before surgery, to after surgery to enhance wound healing and recovery.
Patients should optimize their preoperative nutrition and exercise, while eliminating or minimizing any risk factors for poor wound healing such as smoking, excessive alcohol intake, poor blood sugar control or excessive Body Mass Index (>40 BMI) which all can lead to greater complications after surgery. Immuno-nutrition products such as Ricochet drinks help optimize each patients’ nutritional status for elective surgery. Proper protein and nutritional intake before and after surgery has been shown to improve wound healing and reduce the risk of infection.
During the procedure, Dr. Buechel meticulously cares for the health of the skin and deep tissues throughout the procedure while exposing, retracting, and closing the knee joint, to optimize healing, minimize blood loss, and reduce the incidence of wound healing problems.
A cosmetically appealing scar is common after Dr. Buechel’s procedures because of the variety of techniques he employs during the surgery, and the carefully chosen products he uses for the closure and aftercare. The highest quality suture is used to hold the tissues longer and stronger, while providing anti-bacterial protection. Stratafix Plus barbed antimicrobial suture is our preferred suture.
The outer skin edges are sealed with skin adhesive that blocks out bacteria and provides a waterproof seal to allow showering after surgery. Dermabond skin adhesive is our preferred sealant.
High quality, hypoallergenic, waterproof dressings designed to be gentle on the skin are used to cover the surgical site, adding to the protection of each patients wound.
A Reparel Leg Sleeve is provided after surgery to help control tissue swelling and improve circulation during the early weeks of healing. The sleeves are comfortable, breathable, provide mild compression, are moisture wicking, and anti-microbial, and they use silicon grips at the top band to prevent slippage and folding. The material is composed of synthetic fibers that incorporate finely processed, non-metallic, elemental semi-conductor nanoparticles chosen specifically for their relative efficiency at transmitting energy when body heat contacts the material. The energy is then released as photons, “or particles of light” into the subcutaneous tissues and is thought to promote better cell metabolism /respiration and better circulation by its effects of accelerating the production of ATP in the cell mitochondria.
Cold Therapy wraps devices are critical in wound healing after surgery to reduce swelling and provide non-medication-based pain control. With the use of continuous flow cold therapy sleeves after surgery, patients can use cold as a mechanical way of reducing swelling and pain without the risks of ice packs. These devices allow for longer application without the risks of ice packs.
Dr. Buechel tries to optimize each individuals knee for healing by paying attention to the tissue handling during surgery, the closure technique and materials, and the post-operative wound environment. However, we all heal a little differently. Some people either genetically, due to their muscle tightness, or their adipose tissue thickness, form scar tissue thicker, faster, and tighter, and have wider scars. Some people form very little scar tissue, have more flexible tissue and have very fine line scars. Dr. Buechel uses a variety of techniques to optimize wound healing and appearance for each patient he operates on, hoping for an optimal final result.

Immediate Post-Operative Recommendations
Patients with total knee replacements stay in the hospital ranging from 1-4 nights post-operatively, while the average stay is around 2-3 nights. Patients are discharged from the hospital facility once they are medically stable and have been cleared by the physical therapy staff for safety.
Sterile dressings cover the knee with a mild compression wrap from mid-thigh to mid-tibia when patients leave the operating room. A cooling knee sleeve device is recommended to be used while in bed in the hospital, and when your arrival back at your home, or temporary housing location while you are in town for your surgery and recovery. Patients are recommended to walk each hour for a short distance while awake with support at first, and then without support when they are feeling confident and stable. Many people will use their walker or crutches for 2-3 weeks after total knee surgery.
When resting and not walking during the first two weeks after surgery, the leg should be elevated to heart level or above for swelling reduction, and the cooling sleeve should be on the knee. Pain medications should be taken only as necessary and is made less necessary by using the cooling device and elevating the leg to reduce swelling. A compression stocking is recommended to help control swelling. A specific leg support sleeve that Dr. Buechel has found to be comfortable and promote healthy healing will be provided in the office.
The use of an anticoagulant medication is generally recommended for most patients for at least 3 weeks with the specific choice determined for each patient based on their risk factors. Ankle pumping exercises and frequent short walks daily beginning the day of surgery significantly reduce the risk of blood clots (DVT) along with avoiding tourniquets during surgery, if possible.
Patients will return to the office for a wound check, there outpatient the therapy is instituted, x-rays are reviewed, and concerns are addressed.

Rehabilitation & Recovery Time
A post procedure exercise program is recommended to optimize your outcomes and optimize your quality of life moving into the future. Patients can begin a progressive exercise program the day of surgery. Your therapy begins in the hospital with daily exercises. Local therapists are recommended for patients so they can begin their exercise programs immediately. Those that will be returning to their home towns can take their initial training program plan with them and continue back at home when they arrive.
Most total knee patients begin with an initial 6-week therapy program and often require a second 6-weeks of formal therapy before moving into independent exercise programs.
The initial primary goal is to achieve a well healed incision with full knee extension, so the knee lies flat when extended. The second goal in to maximize flexion. The best judge of final flexion has always been a person’s starting pre-operative flexion range, but this can improve for some with hard work and consistent stretching.
Most people should be able to discontinue pain medications by 3-6 weeks switching to NSAIDs or Acetaminophen only, after this time period. Many people can return to sedentary jobs by 4-6 weeks, sometimes a little earlier, sometimes a little later. Most people can return to light duty work by 6 weeks and some take up to 12 weeks to get back to regular duty level work, if they are in an active job setting with lots of walking, climbing or carrying.
Most patients will say they are starting to feel “pretty good” by 12 weeks. Most say they feel “good” by 6 months. But patients should know that they will improve over the first 12-18 months from the time of surgery at which time patients often begin to be most satisfied.
Total knee replacement is not generally a quick easy recovery for most, but when the surgery is done properly, and the rehabilitation is taken seriously and performed regularly, outcomes are very satisfactory for most patients. The best time to put in your full effort to achieve the best results is the first 3 months after surgery. Therefore, be prepared to put the time in to rehabilitate and train properly after your surgery to optimize your outcome.
Written by: Dr. Frederick Buechel, Jr.
Dr. Buechel is a Stryker certified international instructor and an expert in the field of Robotic-Arm Assisted Knee & Hip Replacement.
Dr. Buechel performs Outpatient Robotic Partial Knee replacement surgery, and Outpatient or short stay Robotic Total Knee replacement in Naples, Florida. Internationally, Dr. Buechel performs Robotic Knee and Hip replacement in Taipei, Taiwan, at Taipei Postal Hospital.
Meet Dr. Buechel